Frog Gut Bacteria "Cures" Colon Cancer 100% in Mice — But Should You Actually Be Excited?
Summary
A team at Japan's JAIST published findings in Gut Microbes showing that Ewingella americana — a bacterium isolated from Japanese tree frog intestines — achieved 100% complete remission in a subcutaneous Colon-26 syngeneic mouse model after a single intravenous injection, with n=3 to n=5 mice per group and no human clinical data; this is explicitly a preclinical proof-of-concept study, not a human cancer treatment. According to a 2024 meta-analysis in PLOS Biology, preclinical cancer treatments reach human regulatory approval at a rate of only approximately 5%, and the average development timeline from animal studies to FDA approval spans 10 to 15 years, meaning even an optimally proceeding program would not reach patients until the mid-2030s at the earliest. A critical safety paradox complicates the path to the clinic: a 2025 case report documented E. americana causing multidrug-resistant sepsis in a 21-year-old cancer patient undergoing chemotherapy, which means the immunocompromised patients who most need a new cancer therapy may be precisely those most vulnerable to the bacterium itself. The study's dual mechanism — selective accumulation in hypoxic tumor microenvironments combined with direct cytolysin-mediated cytotoxicity and T-cell/B-cell/neutrophil immune activation — advances scientific understanding significantly beyond the empirical bacterial cancer treatments of the 19th century, most notably Coley's toxins, by providing a molecular explanation that enables rational engineering and optimization of the approach. The findings simultaneously raise a structural critique of pharmaceutical R&D incentives that have steered four decades of drug discovery away from natural microbiomes, and a pressing conservation argument about the 41% of amphibian species globally facing extinction — a natural chemical library humanity is actively erasing before it can be catalogued.
Key Points
The "100% Complete Remission" Statistic — What It Actually Means
The headline result is factually accurate: Professor Eijiro Miyako's team at JAIST achieved 100% complete remission in their colon cancer mouse model using a single intravenous injection of Ewingella americana, and the paper in Gut Microbes reports this result clearly and without misrepresentation. What the subsequent media coverage almost universally omitted is that this result came from n=3 mice in the initial efficacy experiment and n=5 mice in the comparative efficacy experiment — sample sizes so small that it is statistically impossible to establish a confident estimate of the true underlying remission rate. Early-stage preclinical research routinely uses these cohort sizes; the researchers didn't do anything improper, and the paper itself contextualizes the data appropriately. The problem occurs when "100% complete remission" is lifted from that context and handed to a global audience that includes millions of cancer patients and their families who may make real treatment decisions based on what they read. According to a 2024 PLOS Biology meta-analysis, cancer treatments showing positive animal study results reach human regulatory approval at only about 5%, with oncology-specific market entry rates below 5% and average development timelines from animal studies to FDA approval of 10 to 15 years. The gap between what the headline implies and what the statistical reality of drug development delivers is not merely an academic concern — it shapes patient behavior, affects clinical trial enrollment, and generates false hope that can lead to genuine harm when the anticipated therapy doesn't materialize on the timeline a breathless headline implied.
The Dual Mechanism — Why This Is Categorically Different from Coley's Toxins
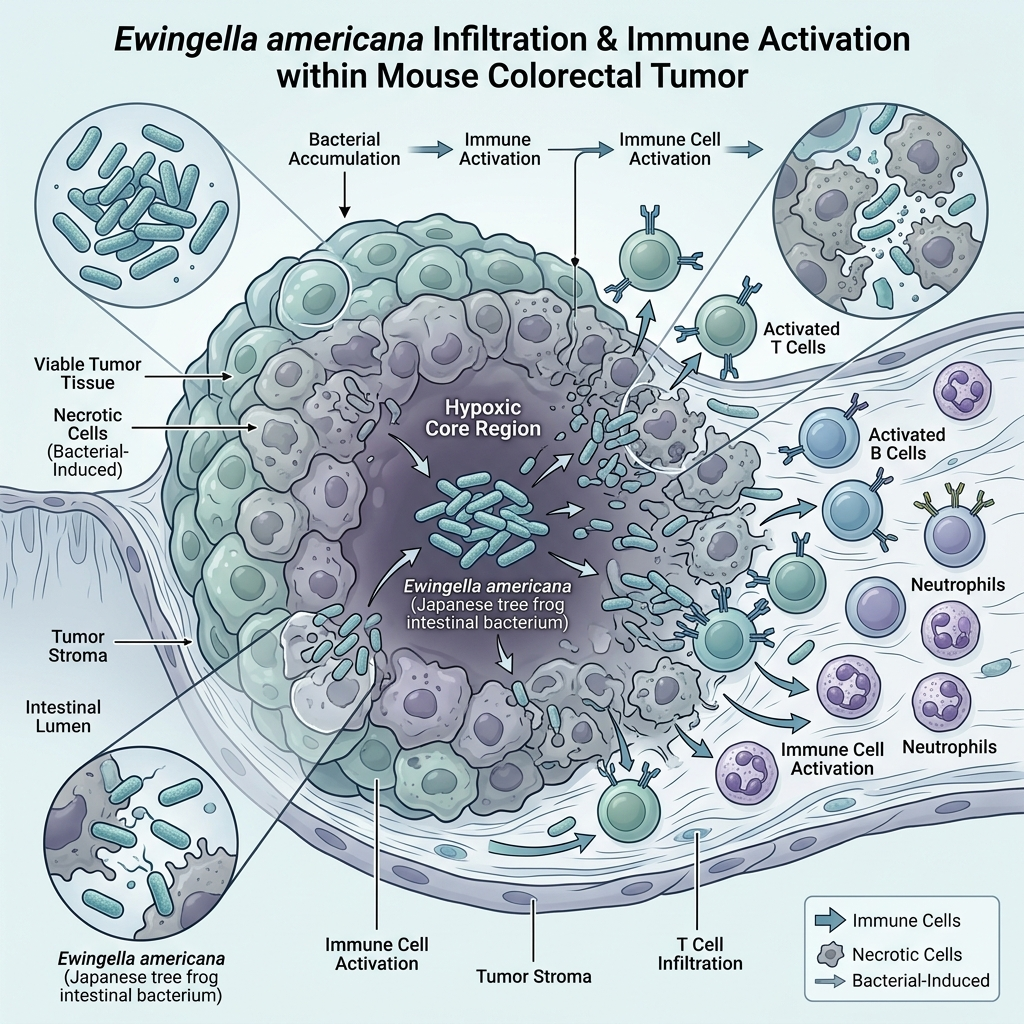
The defining advantage of the JAIST research over the entire prior history of bacterial cancer treatment is not the efficacy result itself but the fact that the mechanism is now understood at the molecular level — and that specificity changes everything about what can be done with this discovery. In 1891, William Coley injected streptococcal toxins into cancer patients and observed remarkable complete remissions in over 10% of more than 1,000 cases, a result that was genuinely extraordinary for the era. Because nobody could explain the mechanism, results were not reliably reproducible across institutions, and when radiotherapy arrived as a seemingly more controllable alternative, Coley's approach was shelved and forgotten for over a century. The JAIST research answers precisely the question that doomed Coley's toxins: E. americana selectively colonizes hypoxic — oxygen-depleted — tumor microenvironments because normal oxygenated tissue cannot support its survival, then attacks through two simultaneous mechanisms — direct cytotoxicity delivered by cytolysin and hemolysin proteins that perforate cancer cell membranes, combined with coordinated activation of T cells, B cells, and neutrophils that generates a broad immune response against the tumor. The rechallenge experiment, in which all ten treated mice rejected reinjected tumor cells 30 days after cure, indicates that immunological memory was formed — the immune system learned to recognize and eliminate these specific cancer cells. Knowing exactly which molecular actors perform which functions means this team can rationally engineer around problems: knock out the LPS gene, amplify the cytolysin expression, add a genetic kill-switch, extract the active proteins for delivery without a live organism. That rational engineering capacity is the foundational difference between a scientific curiosity and a development program with a real clinical future.
The Immunocompromised Patient Safety Paradox — Who Needs It vs. Who Can Tolerate It
The 2025 case report documenting E. americana-induced multidrug-resistant sepsis in a 21-year-old testicular cancer patient receiving chemotherapy is, in my assessment, the single most important and most under-discussed complication in this entire research story. E. americana is a gram-negative member of the Enterobacteriaceae family; in immunocompetent individuals it is rarely pathogenic, but in immunocompromised hosts it functions as an opportunistic pathogen capable of causing life-threatening systemic infection. The JAIST mice were immunocompetent — their intact immune systems cleared the bacteria from the bloodstream within 24 hours while the antitumor effects played out in the tumor microenvironment, a tightly managed sequence that only works if the host's immune clearance function is robust. The population who would actually receive a novel colon cancer therapy consists predominantly of patients with advanced or treatment-resistant disease — people who are already immunosuppressed by prior chemotherapy, radiotherapy, surgical recovery, or disease burden itself. The patients who most desperately need an effective cancer therapy are therefore often the patients whose immune systems are least equipped to safely clear this organism after administration. This is not a manageable side-effect concern at the margins; it is a structural paradox that affects the entire logic of how a clinical trial would be designed, who would be eligible to enroll, and what safety endpoints would be required before efficacy could even be assessed. Solving it demands either genetic engineering to eliminate virulence factors while preserving antitumor activity — which requires those functions to be molecularly separable — or a fundamental shift away from live-organism delivery toward defined protein therapeutics.
The Pharmaceutical Incentive Failure — Why Nobody Looked in a Frog's Gut for 40 Years
The fact that systematic antitumor screening of amphibian gut microbiomes is described as essentially unprecedented in this 2025 paper is, to me, the most structurally revealing finding in the entire study — more revealing than the 100% complete remission rate itself. Modern pharmaceutical drug discovery is organized around synthetic chemical libraries and high-throughput screening because synthetic compounds are unambiguously patentable, manufacturable at industrial scale, and recoverable through multi-decade exclusivity windows that justify the billions spent on clinical development. Natural microbial isolates from wildlife species don't fit that model: their IP protection is narrower, their manufacturing at clinical scale is considerably more complex, and their regulatory pathway as live biological products is more uncertain than for small molecules. The result has been a rational — but scientifically costly — four-decade absence of economic motivation to explore what hundreds of millions of years of amphibian evolution has assembled in the gut microbiomes of 8,000 species. The JAIST team screened just 45 species and found nine antitumor-active bacteria — a 20% hit rate that implies this space may be extraordinarily rich. I think this constitutes one of the clearest examples of market failure in modern drug development: a scientific opportunity of enormous potential value that the private sector had no financial incentive to pursue. Correcting this may require public funding mechanisms that explicitly reward natural-compound exploration independent of immediate IP outcomes, because the current system's incentive structure will otherwise continue pointing researchers in the wrong direction.
Amphibian Extinction and the Natural Pharmacy We Are Erasing in Real Time
E. americana's discovery from the gut of a Japanese tree frog — one of 45 species screened in a single study — lands against a backdrop that should give the global scientific community serious pause. The IUCN's 2023 Second Global Amphibian Assessment reports that 41% of amphibian species worldwide face extinction threats, the highest proportion of any vertebrate group on Earth; of roughly 8,000 known species, 2,873 are under simultaneous pressure from chytrid fungal disease, habitat destruction, and accelerating climate change. The JAIST team found nine antitumor-active bacteria from 45 species — a 20% hit rate suggesting that the vast majority of the world's amphibian species harbor unstudied gut microbiomes that may contain additional therapeutic candidates of comparable or greater potency. Some of those species are being lost right now, before any researcher has had the opportunity to screen them, taking their microbiomes permanently into extinction. This transforms the biodiversity conservation argument from a purely ethical imperative into an immediately practical one with direct economic implications: losing amphibian species is not merely an ecological tragedy, it is the permanent destruction of pharmaceutical assets that evolution spent hundreds of millions of years developing and that humanity's current R&D incentive structure never thought to study. The scientific community, pharmaceutical industry, and conservation policy world have rarely had a more direct and concrete argument for connecting drug discovery investment to species preservation — and this research makes that argument in the most vivid terms possible.
Positive & Negative Analysis
Positive Aspects
- Molecularly Understood Mechanism Enables Rational and Targeted Drug Development
The most important distinction between E. americana and the entire prior history of bacterial cancer treatment is that researchers now know exactly why this organism kills tumors — and that mechanistic clarity is what separates a potentially developable therapy from an empirical curiosity. The bacterium selectively accumulates in hypoxic tumor microenvironments, produces cytolysin and hemolysin proteins that directly destroy cancer cells, and simultaneously activates T cells, B cells, and neutrophils to mount a coordinated immune response. When problems arise in translational medicine — as they always do — a team that understands the specific molecular actors has rational engineering handles: they can knock out the LPS gene to reduce endotoxin toxicity, increase cytolysin expression to allow lower bacterial doses, engineer a genetic kill-switch element to address immunosuppressed-patient safety, or extract the active secreted proteins for delivery without a live organism. The same molecular understanding that explains the 100% preclinical remission rate is what makes this discovery substantively more than a footnote, and it is the reason the research program deserves serious development investment regardless of whether E. americana as a live organism ultimately reaches the clinic.
- Single-Injection Efficacy Could Transform How Cancer Treatment Is Delivered
If the single-injection complete remission finding survives translation to human biology — a significant "if" — the implications for treatment delivery would be profound. Conventional chemotherapy requires multiple infusion cycles over months, with each session carrying cumulative toxicity, demanding hospital infrastructure, and consuming patient time and energy that is already limited. Immune checkpoint inhibitors are typically administered every two to three weeks over an extended period with repeated monitoring visits. E. americana achieved complete remission in every tested mouse from a single dose and outperformed both liposomal doxorubicin given four times and anti-PD-L1 given four times. A single-infusion cancer therapy would dramatically reduce the per-patient treatment burden, cut required clinic visits, limit cumulative toxicity, and make the therapy practically deployable in health systems where multi-session treatment protocols are logistically impossible. This advantage is speculative until human data exists, but the preclinical direction points toward a treatment experience categorically different from current standard of care — and for patients managing cancer treatment alongside work, family, and the physical demands of illness, that difference is not trivial.
- Immunological Memory Formation Points Toward Durable Long-Term Relapse Prevention
The rechallenge experiment in the JAIST paper may be the most clinically significant result in the entire study. Thirty days after successful primary treatment, researchers reinoculated treated mice with the same Colon-26 cancer cells — and all ten rechallenge mice rejected the new tumors completely. This demonstrates that E. americana did not merely eliminate the presenting tumor but educated the immune system to recognize and destroy these cancer cells on future encounters — a durable immunological memory response. Relapse and metastatic recurrence represent among the most feared outcomes in colon cancer treatment; the median survival for metastatic colorectal cancer with current best-available therapies remains approximately 30 months, making durable immune protection a clinically meaningful goal. Existing immune checkpoint inhibitors achieve lasting responses in roughly 20 to 40% of patients where they are effective, and those are considered exceptional results. E. americana produced immunological memory in 100% of treated preclinical subjects. The species gap between mouse and human immune memory is real and must not be assumed away, but the mechanistic basis — T-cell and B-cell activation generating antigen-specific memory — is conserved across mammals, and it makes this a high-priority question for any future human safety study.
- Opens an Entirely Untapped Drug Discovery Frontier in Amphibian and Reptile Microbiomes
Beyond its value as a specific drug candidate, E. americana's discovery establishes that systematic antitumor screening of amphibian gut bacteria is viable, productive, and currently operating at essentially zero coverage of the available biological space. The JAIST team identified nine antitumor-active bacterial strains from just 45 species — a roughly 20% hit rate that, if it scales across the broader universe of 8,000 amphibian and 12,000-plus reptile species, implies the existence of thousands of unstudied therapeutic candidates. This is not incremental optimization of existing drug platforms but the opening of an entirely new chemical library that evolution has been assembling for hundreds of millions of years. Some organisms in that library may produce compounds active against cancers where current therapies have largely failed — pancreatic cancer, glioblastoma, treatment-resistant ovarian cancer — that synthetic library screening has been unable to address. The JAIST paper provides both the proof-of-concept and a replicable methodological template for a systematic global survey. If that survey attracts the funding and institutional support it deserves before further extinction closes the window, the long-term drug discovery impact could substantially exceed whatever E. americana achieves on its own.
- Head-to-Head Preclinical Data Outperforms Established Standard-of-Care Agents in Controlled Comparison
One of the most scientifically compelling aspects of the JAIST paper is the direct comparison design: rather than demonstrating E. americana's efficacy in isolation, the researchers ran it against liposomal doxorubicin — a standard chemotherapy agent used in colon cancer management — and anti-PD-L1 antibody, one of the most widely deployed immune checkpoint inhibitors. E. americana at a single dose produced 100% complete remission while liposomal doxorubicin at four doses achieved zero complete remissions and anti-PD-L1 at four doses achieved one complete remission. These comparisons were conducted within the same experimental model under identical conditions, making this a genuine within-study head-to-head result rather than a cross-study extrapolation subject to confounding variables. Outperforming established standard-of-care agents in a controlled preclinical comparison is a meaningfully high bar that most drug candidates fail to clear — it is precisely the kind of result that generates legitimate scientific attention and justifies investing development resources in the next stage of validation. This does not mean E. americana will outperform these agents in humans; the specific Colon-26 syngeneic model has known limitations in predicting human response. But the result strongly supports the conclusion that the antitumor activity here is real and substantial, not marginal or artifactual.
Concerns
- Gram-Negative Endotoxin Poses a Real and Well-Documented Systemic Toxicity Risk
E. americana is a gram-negative bacterium in the Enterobacteriaceae family, meaning it carries lipopolysaccharide in its outer membrane, and intravenous administration of gram-negative bacteria creates a clinically significant septic shock risk in humans. Mice are substantially less sensitive to LPS than humans on a weight-adjusted basis, meaning the absence of acute toxicity observed in the JAIST mouse study does not reliably predict human safety at equivalent doses. A comprehensive 2018 peer-reviewed review of bacterial cancer therapy (PMC5810261) explicitly identifies gram-negative LPS endotoxin toxicity as a primary barrier to the clinical translation of this entire class of treatments, and the concern is not theoretical — it is based on decades of failed attempts to use gram-negative organisms therapeutically in human patients. Engineering solutions include LPS-deficient knockout strains, lipid A structural modification, or replacement of the whole-organism approach with purified secreted protein fractions, but each of these approaches requires 12 to 18 months of additional preclinical safety validation at minimum before any human study could be contemplated. Until the LPS problem is resolved at a clinical safety standard applicable to immunologically diverse human patients, intravenous E. americana administration in humans remains a research-stage question with no clear timeline for resolution.
- Tiny Sample Sizes Make Statistical Confidence Fundamentally Unavailable at This Stage
The central result of the JAIST study — 100% complete remission — rests on an initial efficacy cohort of n=3 mice and a comparative efficacy cohort of n=5 mice. These sample sizes are not unusual for early exploratory preclinical work, and their use reflects standard practice rather than methodological error. What they mean statistically, however, is that the true underlying complete remission rate could be anywhere from roughly 50% to 100% and remain consistent with the observed data — statistical confidence intervals at this sample size span that entire range. An independent laboratory running the same protocol in a cohort of n=20 mice might find a 65% CR rate, which is still an impressive and publishable result but a profoundly different clinical prospect than the headline implied. The 2024 PLOS Biology meta-analysis on translational medicine found that small-sample preclinical studies systematically overestimate effect sizes due to random variation and publication bias, and this is a well-characterized contributing factor to the 5% preclinical-to-approval success rate in oncology. Until independent replication with substantially larger cohorts confirms both that the antitumor effect is real and what its actual magnitude is in a properly powered study, the 100% figure should be understood as a promising upper bound rather than a confirmed efficacy estimate.
- Subcutaneous Tumor Model Introduces Important Biological Differences from Real Colon Cancer
The experimental model used in the JAIST study implanted Colon-26 cancer cells under the skin of BALB/c mice — a subcutaneous setup that is standard for initial antitumor screening because it is technically simple and allows easy tumor measurement, but which differs from actual colon cancer biology in several important respects. Real colon cancer grows within the epithelial lining of the colon, embedded in a tissue microenvironment with its own resident immune populations, mucus barrier, stromal components, local vascular architecture, and specific patterns of immune cell infiltration and suppression. The tumor's internal hypoxia gradients, which are central to E. americana's proposed mechanism of selective accumulation, differ meaningfully between a subcutaneous mass and an orthotopic colon tumor. The authors acknowledged this limitation explicitly in the paper, noting that orthotopic models would be a necessary next step before drawing strong conclusions about clinical applicability. Success in a subcutaneous model does not guarantee success in an orthotopic model, and the oncology literature contains many examples of agents that performed well subcutaneously but failed when tested in the anatomically and biologically appropriate setting. Convincing orthotopic model data is a required next step before this research program can credibly claim clinical translation potential.
- Narrow Therapeutic Window Creates Significant Challenges for Clinical Dose Management
The JAIST dose-response characterization found that the maximum tolerated dose and the maximum efficacy dose in their model were essentially the same value, indicating a narrow therapeutic window. In clinical pharmacology, a narrow therapeutic window means the margin between a dose that produces adequate therapeutic effect and a dose that causes unacceptable toxicity is small — and managing this margin in a human patient population is considerably more challenging than in an inbred mouse colony where body weight, organ function, and immune status are far more uniform than in clinical practice. Real cancer patients vary substantially in body weight, kidney and liver metabolic capacity, baseline inflammatory status, and immune function, all of which affect the pharmacokinetics and pharmacodynamics of an administered bacterial agent. A dose that is simultaneously safe and effective in one patient subgroup might be sub-therapeutic in another or dangerously toxic in a third. The authors acknowledged this limitation explicitly and identified expanding the therapeutic window as a prerequisite to clinical development. Solving this will likely require engineering a higher-potency, lower-dose bacterial variant, developing pre-administration biomarkers that allow individualized dosing, or identifying patient selection criteria that restrict use to those whose physiology accommodates the available dose range — all of which add significant time and cost to the development program.
- Immunocompromised Patient Safety Paradox Threatens the Core Clinical Target Population
This is the deepest and structurally most difficult challenge facing the E. americana program. The patients who would benefit most from a new colon cancer therapy — those with advanced or treatment-resistant disease who have exhausted standard options — are frequently immunocompromised by prior chemotherapy, radiotherapy, biological therapy, or the disease itself. A 2025 Turkish case report documented E. americana causing multidrug-resistant sepsis in a cancer patient receiving chemotherapy, demonstrating that the bacteria which clears harmlessly from an immunocompetent mouse in 24 hours can cause life-threatening systemic infection in a real cancer patient whose immune clearance function is impaired. The entire safety logic of the JAIST protocol depends on robust host immune function performing rapid bacterial clearance while the antitumor effects play out in the tumor microenvironment — but the target patient population systematically lacks the immune function that makes this safe. If E. americana's therapeutic mechanism and its sepsis-causing capacity share molecular machinery, engineering one out necessarily compromises the other, and there is no engineering solution that avoids a genuine scientific dead end. Even if the functions can be separated, validating that separation requires years of additional preclinical work in immunosuppressed large-animal models before any human safety study is ethically possible. I believe this paradox, not the LPS problem or the sample size limitations, is the single most important translational barrier this research must overcome.
Outlook
Let me lay out what I actually think happens next — short-term, mid-term, and long-term. I'll be direct: I'm cautiously optimistic, but the weight of that caution is real. The science is solid, the mechanism is elegant, and this research arrives at a moment when the microbiome oncology field is well-funded and actively looking for exactly this kind of candidate. But between a clean preclinical mouse study and a validated human therapy stretches one of the longest and most unpredictable obstacle courses in modern medicine, and this research faces several obstacles that are harder than typical.
In the next one to six months, the most consequential development won't come from JAIST itself — it will come from independent laboratories attempting to replicate the findings. The paper appeared online in Gut Microbes in late 2025 and broke into mainstream science media coverage in July 2026, meaning the global research community is now paying serious attention. I'd expect at least two or three independent groups to announce replication attempts using different mouse models within the coming months. Replication is the study's first critical checkpoint. The original n=3 to n=5 cohort sizes make it statistically impossible to confidently estimate the true underlying complete remission rate. If independent labs running cohorts of n=10 to n=20 find CR rates of 65–80%, that is still a remarkable and publishable result — but it reframes the "100% cure" narrative considerably and sets more realistic expectations for what might eventually reach the clinic.
Simultaneously, Professor Miyako's team is almost certainly running two essential follow-up experiments. The first is an orthotopic colorectal cancer model — tumor growing inside the actual colon rather than implanted subcutaneously — to determine whether the hypoxic accumulation mechanism operates with equivalent efficiency in a colon-sited tumor. The authors acknowledged this gap explicitly in the paper. The second follow-up is testing efficacy against other major solid tumor types: breast, lung, pancreatic, and hepatocellular carcinoma are the obvious targets. If E. americana works broadly across solid tumors, not just in the specific Colon-26 model, the research program's addressable market grows enormously and attracts proportionally more development resources.
Between six months and two years, the research enters its most technically demanding phase, and two pivotal engineering questions will define the trajectory. The first is the gram-negative endotoxin problem. E. americana carries lipopolysaccharide in its outer membrane, as all gram-negative bacteria do, and intravenous administration of gram-negative organisms creates a real septic shock risk in humans, who are far more sensitive to LPS than mice. A 2018 peer-reviewed review of bacterial cancer therapy identified gram-negative LPS toxicity as a central barrier to this entire class of clinical translations. Engineering solutions include creating LPS-deficient attenuated strains through gene knockout, extracting and purifying the active antitumor secreted proteins for delivery without the live organism, or pre-treating patients with LPS-neutralizing agents before infusion. Each approach is scientifically feasible, but each requires 12 to 18 additional months of preclinical safety validation before any human study becomes possible.
The second mid-term question — which I consider more fundamental — is the immunocompromised patient safety paradox. The patients who would first receive a new colon cancer therapy are predominantly those with progressive disease, meaning they are immunosuppressed from prior chemotherapy or radiotherapy. The 2025 Turkish case report demonstrated that E. americana causes drug-resistant sepsis in exactly that population. The JAIST mice were immunocompetent, and their intact immune function cleared the bacteria within 24 hours. In an immunosuppressed patient, that clearance mechanism is impaired. Resolving this paradox likely requires genetic engineering to insert a kill-switch element — a bacterial gene triggering self-destruction in response to an administered antibiotic — combined with comprehensive safety testing in immunosuppressed non-human primates. This is technically achievable using modern synthetic biology tools, but it adds years to the development program and requires demonstrating that the kill-switch doesn't compromise antitumor efficacy.
The mid-term period also unfolds against a favorable commercial backdrop. Grand View Research projects the global microbiome therapeutics market to grow from $94.9 million in 2022 to $1.07 billion by 2030, at a 35.3% compound annual growth rate, with oncology applications representing the fastest-growing segment at 36.33% CAGR. This market environment creates real commercial interest in exactly the kind of asset E. americana represents. If independent replication holds and a clear engineering path around the LPS and immunosuppression problems emerges, the JAIST team could attract partnership interest through a spinout company or licensing agreement with an established biotech. The intellectual property challenge — natural-origin bacterial strains are harder to protect broadly than synthetic molecules — remains a structural friction point, but it is solvable with creative IP strategy, particularly if the active secreted proteins can be characterized and patented as defined pharmaceutical entities.
Looking two to five years out, I see three distinct scenarios. In the optimistic scenario, which I'd place at roughly 15 to 20% probability, independent replication confirms strong antitumor activity across multiple solid tumor models and in orthotopic settings. An engineered attenuated strain with deleted LPS and a validated kill-switch clears non-human primate safety studies. An IND application is filed around 2028–2029, and Phase I clinical testing begins with dose escalation in immunocompetent early-stage solid tumor patients, using hypoxia imaging to confirm that the selective tumor accumulation mechanism operates in humans. Clean Phase I data supports Phase II expansion for colon cancer around 2031–2032. This scenario requires every technical obstacle to resolve on the optimistic end of its range, but it is not beyond reach given the strength of the mechanism data and the C. novyi-NT precedent showing that this class of therapy can clear human safety studies.
In the base case scenario — around 45 to 50% probability — independent replication partially succeeds, with CR rates of 60 to 75% in larger cohorts. The engineering challenges prove more complex than anticipated, particularly around immunocompromised patient safety, and clinical entry of E. americana as a live organism is ultimately superseded by its derived active compounds. This follows the established pattern of most successful natural-product drug discoveries: the source organism identifies the mechanism and the therapeutic direction, but the final drug is a purified protein, a defined recombinant biologic, or a synthetic analog rather than the wild organism itself. A secreted-protein therapeutic with known molecular identity, defined pharmacokinetics, and a scalable manufacturing process is far easier to move through clinical development than a live bacterial product. In this scenario, Phase I entry shifts to 2031–2033, and any regulatory approval is a 2035-or-later story at best.
In the pessimistic scenario — roughly 30 to 35% probability — one or both principal barriers proves unresolvable. The specific concern I keep returning to is the possibility that E. americana's cancer-killing activity and its sepsis-causing capacity are mediated by overlapping molecular machinery. If the proteins responsible for direct tumor cytotoxicity are the same proteins that drive opportunistic infection in immunocompromised hosts, then removing the dangerous components also eliminates the therapeutic ones. That would be a genuine scientific dead end, not a solvable engineering problem. A separate concern involves the species gap in immunology: this research depends heavily on immune activation, and human immune systems differ from mouse immune systems in cytokine profiles, T-cell subset distributions, and tumor microenvironment suppression mechanisms in ways that have consistently caused compelling mouse results to fail in humans. In the pessimistic scenario, E. americana joins the substantial majority of preclinical cancer therapies that worked in mice and could not be translated to people.
Whatever the ultimate fate of E. americana as a specific drug candidate, one consequence of this research is already irreversible: it has credibly established amphibian gut microbiomes as an underexplored frontier of anticancer compound discovery. The JAIST team screened 45 species and found nine antitumor-active bacterial strains — roughly a 20% hit rate, extraordinary by any standard. There are roughly 8,000 amphibian and over 12,000 reptile species on Earth, the vast majority with entirely unstudied gut microbiomes. If this paper catalyzes a systematic global survey of those organisms before further extinction narrows the opportunity, the long-term impact on the oncology drug discovery pipeline could far exceed whatever outcome E. americana achieves on its own. That possibility — and the 41% extinction rate that threatens to close the window on it — is the most urgent takeaway this research offers, and I think the scientific community should be making the argument for amphibian conservation loudly on the back of these findings.
Sources / References
- Iwata S, Yamasita N, Asukabe K, Sakari M, Miyako E. Anticancer therapy using a gut bacterium derived from amphibians and reptiles. Gut Microbes. 2025;17(1):2599562 — Gut Microbes (PMC)
- JAIST Press Release. JAIST researchers find gut bacteria from frogs can eliminate cancer tumors. EurekAlert (AAAS) — EurekAlert
- Hooijmans CR et al. Translation of animal research to clinical practice. PLOS Biology 2024 — PLOS Biology
- E. americana sepsis in immunocompromised cancer patient. Cureus 2025 — Cureus (PMC)
- Phase Ib Study: Pembrolizumab + Clostridium novyi-NT in Advanced Solid Tumors. Clinical Cancer Research 2025 — Clinical Cancer Research (AACR)
- Bacterial Therapy of Cancer: Promises, Limitations, and Insights for Future Directions. PMC Review — PMC
- IUCN 2023 Second Global Amphibian Assessment — IUCN
- Global Microbiome Therapeutics Market 2022-2030 — Grand View Research