They Called It Impossible for 40 Years — Here's Why I'm Both Thrilled and Furious
Summary
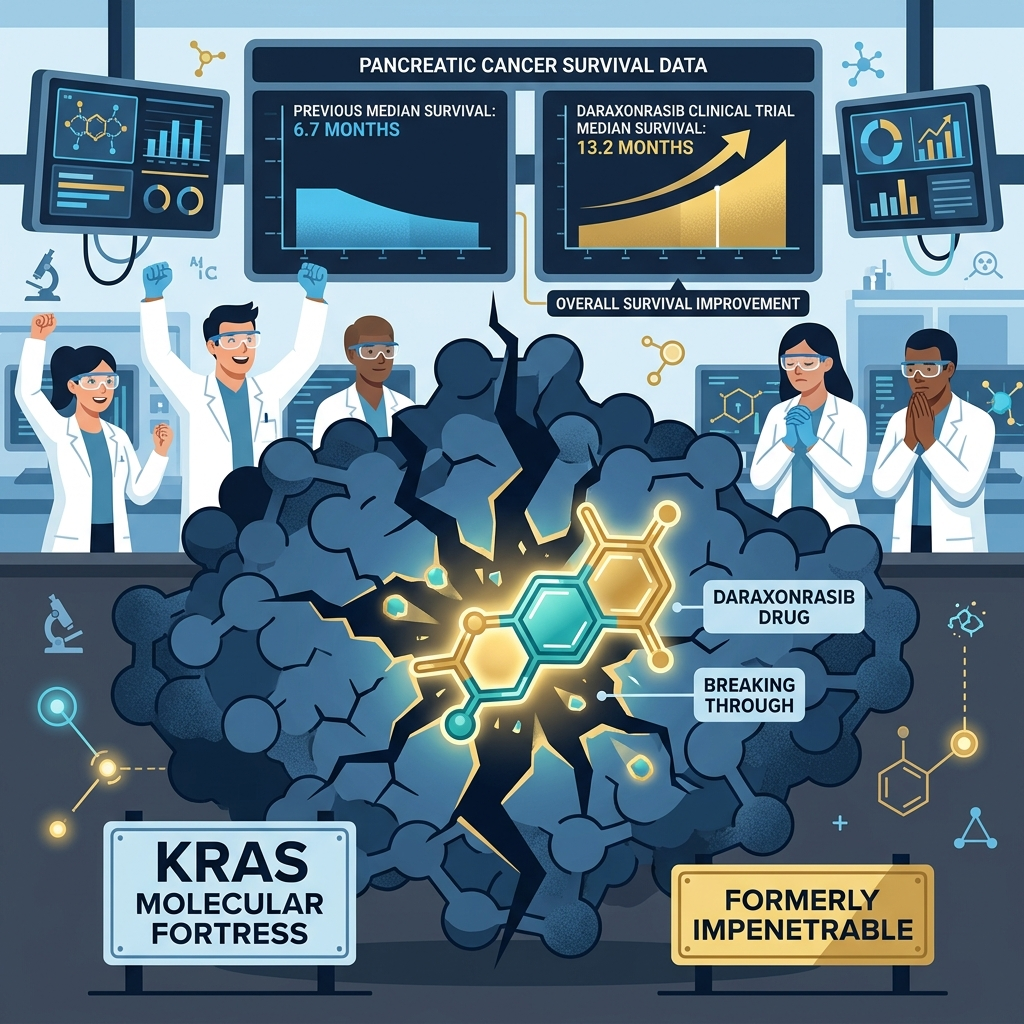
Daraxonrasib, the world's first broad-spectrum oral RAS(ON) inhibitor targeting the previously "undruggable" KRAS oncogene, was unveiled at ASCO 2026 as a transformative advance in metastatic pancreatic cancer treatment, drawing a standing ovation after the Phase 3 RASolute 302 trial demonstrated a near-doubling of median overall survival. Across 501 previously treated patients, the trial reported median overall survival of 13.2 months on daraxonrasib versus 6.7 months on chemotherapy — a hazard ratio of 0.40 (p<0.0001), representing a 60% reduction in death risk, with one-year survival rising from 18.7% to 53.3%, marking the first time any second-line agent had pushed median survival past one year in this indication. Unlike sotorasib, which targets only the KRAS G12C variant accounting for just 1–2% of pancreatic cancers, daraxonrasib simultaneously suppresses G12D (40%), G12V (29%), and G12R (15%) — the three mutations responsible for the overwhelming majority of KRAS-driven pancreatic cancer — establishing the proof of concept for broad-spectrum RAS inhibition as a viable therapeutic strategy. This clinical triumph, however, coexists with a structural contradiction: the projected monthly price of $30,547–$37,318 renders the drug effectively inaccessible to 85–90% of the 510,922 annual global pancreatic cancer patients, and the 31-year gap between KRAS discovery in 1982 and the NCI RAS Initiative's launch in 2013 exposes a long history of underfunding — $8,945 in NCI per-death research spending for pancreatic cancer versus $69,800 for breast cancer — that deserves as much attention as the breakthrough itself. Treatment effects vary significantly by individual, and as daraxonrasib is currently available only through expanded access prior to formal FDA approval, all treatment decisions must be made in consultation with a qualified oncologist.
Key Points
40 Years of "Impossible" — Science's Achievement and the System's Confession
KRAS was first identified as an oncogene in 1982 and within a decade was recognized as the mutation driving 25–30% of all human cancers and 90–95% of pancreatic cancers — arguably the most common oncogenic driver in human malignancy — yet its unusually smooth protein surface and picomolar-affinity GTP binding (documented in Cancer Biology & Medicine) made it effectively immune to small-molecule drug targeting for four decades, while indirect strategies like farnesyltransferase inhibitors failed in the clinic because KRAS simply routed around the blockade through alternative enzyme pathways. The National Cancer Institute did not establish a dedicated RAS research initiative until 2013 — 31 years after the gene's discovery — yet a successful Phase 3 trial arrived just 13 years after that concentrated funding commitment began. A 2025 PMC study captures the funding disparity with uncomfortable precision: NCI spent $69,800 in research per annual breast cancer death and just $8,945 per annual pancreatic cancer death, despite pancreatic cancer killing more than twice as many Americans each year. I believe the "undruggable" label functioned partly as a scientifically accurate description of what happens when a genuinely difficult problem is inadequately funded, and partly as a justification for not prioritizing a disease that lacked the advocacy infrastructure and survivor community scale that attracted sustained public investment to other cancers. Daraxonrasib's success is as much a story of what becomes possible when resources finally arrive as it is a story of molecular ingenuity, and the 31-year gap between discovery and serious investment represents preventable delay — not inevitable scientific destiny — a distinction that demands accountability, not just celebration.
HR 0.40 — A Number This Field Has Never Seen Before
The Phase 3 RASolute 302 trial reported a hazard ratio of 0.40 for overall survival, meaning daraxonrasib reduced the risk of death by 60% compared to standard chemotherapy — a magnitude of benefit that is genuinely rare in oncology, with no prior precedent in metastatic pancreatic cancer at the second-line setting or any other. Published in the New England Journal of Medicine, the full trial data show statistical significance at p=5.9×10⁻¹⁰ for the RAS G12 mutation subgroup and p=4.6×10⁻¹¹ for the full trial population — significance so overwhelming that it removes any statistical doubt about the underlying effect. Progression-free survival also roughly doubled from 3.5 months on chemotherapy to 7.3 months on daraxonrasib (HR 0.45), and the one-year survival rate rose from 18.7% to 53.3% — the first time any second-line agent has pushed that rate above 50% in this indication. Dana-Farber Cancer Institute's Dr. Brian Wolpin, the trial's principal investigator, noted that this represents "the first RAS inhibitor to be evaluated in a large randomized trial for pancreatic cancer patients" — a foundational milestone, not merely a data point, establishing that RAS inhibition can produce clinically transformative outcomes in this disease for the first time. The clinical weight of these numbers becomes fully clear only when you recall that before this trial, no second-line treatment had ever achieved a median overall survival exceeding one year in metastatic pancreatic cancer — daraxonrasib didn't just improve on the prior standard, it expanded what the standard was thought capable of producing.
The Duality of 13.2 Months — Milestone and Limitation at Once
Let me be direct about why this part of the story is the hardest to tell honestly: 13.2 months is a remarkable clinical achievement in a disease where median second-line survival had never crossed one year before, and the emotional response from oncologists at ASCO — Dr. Julie Gralow calling it "more than a home run — a grand slam" and Dr. Rachna Shroff saying she "started crying in the clinic" — is a legitimate expression of 40 years of scientific frustration finally finding its breakthrough moment. But two other voices deserve equal prominence in this story: Dr. Anirban Maitra at NYU Langone Health, who has been emphatic that "this is not a cure, we have not cured pancreatic cancer, I cannot emphasize this enough," and Dr. Elizabeth Jaffee at Johns Hopkins, who noted that despite decades of developing new therapies, pancreatic cancer "is still a death sentence." I believe both sets of reactions need to coexist in honest coverage of this moment, because the extra seven months this drug provides are genuinely meaningful — quality-of-life data showing pain worsening HR 0.51 and QoL improvement HR 0.60 confirm they are livable months — but a diagnosis of metastatic pancreatic cancer in 2026 still carries a median horizon of approximately one year. When "survival doubled" headlines risk being read as "problem solved," patients and families are set up for a version of hope the evidence cannot fully deliver, and calibrated honesty about what 13.2 months means is more valuable than any amount of institutional enthusiasm.
The Accessibility Paradox — A $37,000/Month Revolution for Whom?
Revolution Medicines completed a $2.225 billion stock offering immediately following the ASCO plenary presentation — originally targeting $1 billion, they doubled it post-data, ultimately raising $1.725 billion in equity plus $500 million in convertible notes — driving the company's market capitalization to $29 billion, with the stock having risen approximately 10-fold from its IPO lows. The Stifel analyst estimate places daraxonrasib's monthly price at $30,547–$37,318, or $237,556–$269,051 annually — nearly double the monthly cost of the prior KRAS inhibitor sotorasib, with the premium positioned around broader mutation coverage and dramatically superior survival data relative to standard second-line chemotherapy. But the global arithmetic is stark: of the 510,922 people diagnosed with pancreatic cancer worldwide in 2022 (Journal of Global Health), the 85–90% concentrated in low- and middle-income countries face a systematic review finding from Frontiers in Public Health that 57.7% of anti-cancer medicines are entirely out-of-pocket expenses, with 8.3% not available at all; in Bangladesh, where 84% of households earn $2–9 per day, average cancer treatment costs total $3,234 per treatment course — a $37,000 monthly drug simply does not exist in that economic reality as a treatment option. Nature Reviews Clinical Oncology has documented that more than 50% of WHO essential medicines list anti-cancer drugs are already inaccessible in low- and middle-income countries; daraxonrasib, at its projected price, will exceed that accessibility threshold by an order of magnitude. I don't think this is an argument against innovation — I think it is an argument for recognizing that a breakthrough accessible only to the citizens of wealthy countries is structurally incomplete, and that the substantial public investment enabling this drug creates an obligation toward global access that the current pricing model does not honor.
Resistance — The Ticking Clock Testing Every Grand Claim
No matter how impressive the RASolute 302 data is, the question of how long the response lasts will ultimately define daraxonrasib's real-world impact — and early evidence already shows that the clock is ticking. Research presented at AACR has documented acquired resistance mechanisms in patients on daraxonrasib monotherapy: KRAS gene amplification observed in three patients, MAP2K1/2 mutations in five patients, and PI3K/MTOR pathway alterations in four patients, alongside preclinical evidence of KRAS Y64X and Y71H secondary mutations, Myc amplification, and RAF dimerization changes that may represent additional clinical resistance routes. These resistance mechanisms predominantly operate through reactivation of the RAS–MAPK signaling pathway, and in cases involving receptor tyrosine kinase upregulation, they may require combination strategies targeting EGFR or MET to suppress the most active escape pathways. A 2026 paper published in Cell identified molecular glue complex disruption as a resistance mechanism that may apply not just to daraxonrasib but to the entire class of RAS(ON) inhibitors — a structural concern that extends beyond any individual molecule. The current 13.2-month median overall survival reflects single-agent performance in a trial population that has not accumulated enough follow-up time to fully reveal what the durable response profile looks like, and whether the survival benefit concentrates in a biomarker-identifiable responder subpopulation will only be known through longer follow-up data unavailable before 2028 or later. I think this means the "game changer" label should be held as conditional — fully valid as a proof of concept and as a first step, but genuinely contingent on combination strategies successfully managing the resistance pathways that have already been identified in early post-approval experience.
Positive & Negative Analysis
Positive Aspects
- A 60% Reduction in Death Risk — Data That Stands Alone
The HR 0.40 result in RASolute 302 is the most powerful survival signal ever recorded in second-line metastatic pancreatic cancer, and it stands up to scrutiny at every statistical level: significance at p=4.6×10⁻¹¹ for the full population, one-year survival improving from 18.7% to 53.3%, and progression-free survival doubling from 3.5 to 7.3 months. Before this trial, no second-line agent had ever pushed median overall survival past one year in this disease — daraxonrasib didn't just clear that threshold, it approached two years in responder subgroups while nearly doubling what the prior chemotherapy standard achieved. The magnitude of these results is not incremental improvement; it represents a qualitative expansion of what second-line pancreatic cancer treatment is capable of producing, establishing a new clinical benchmark that all future second-line agents will need to meet or exceed. The correlation between the survival benefit and patient-reported quality-of-life improvement (QoL HR 0.60) confirms that the additional months represent genuinely livable time — not mere calendar extension purchased at the cost of worse suffering. If this magnitude of effect extends to the first-line setting — which RASolute 303 is designed to determine — the clinical implications compound further and could position daraxonrasib as the most impactful oncological development in a generation.
- Oral Dosing Plus Better Tolerability Than Chemotherapy
Daraxonrasib's delivery mechanism — a daily oral tablet rather than intravenous infusion — eliminates the hospitalization burden, infusion center scheduling, IV access requirements, and travel demands that characterize standard chemotherapy, representing a meaningful improvement in the day-to-day quality of treatment for patients already managing a serious illness. The safety data reinforces this advantage: Grade 3 or higher adverse events occurred in 43.6% of daraxonrasib patients versus 57.5% on chemotherapy, meaning the more effective drug also produced fewer serious toxicities — an unusual combination in oncology where more powerful agents typically carry more severe side-effect profiles. Treatment discontinuation rates were 1.2% for daraxonrasib versus 11.2% for chemotherapy — essentially a nine-fold difference in treatment-ending adverse events — which is clinically critical for patients trying to complete a full treatment course rather than having their therapy terminated by intolerable side effects. The main new adverse events associated with daraxonrasib, rash affecting 86% of patients (grade 3+ in 14%) and stomatitis affecting 54% (grade 3+ in 12%), require active monitoring and management but are substantially more manageable for most patients than the cumulative toxicity burden of standard chemotherapy regimens. Dr. Pashtoon Kasi at Fred Hutchinson Cancer Center reported observing patient improvement in pain and tumor markers within just one to two weeks of starting treatment — a speed of clinical response that is unusually rapid for a drug in this indication and speaks to the mechanism's on-target efficacy.
- The First Broad-Spectrum RAS Inhibitor — A Paradigm Shift, Not an Upgrade
Prior KRAS-targeted drugs, including sotorasib and adagrasib, addressed only the G12C variant — a mutation that appears in 10–15% of KRAS-mutant lung cancers but just 1–2% of pancreatic cancers, leaving the overwhelming majority of pancreatic cancer patients without any RAS-targeted option regardless of their individual mutation profile. Daraxonrasib simultaneously suppresses G12D (40% of pancreatic KRAS mutations), G12V (29%), and G12R (15%), which together represent the vast majority of KRAS alterations in this disease — establishing it as the first drug to cover this mutational breadth as a single daily oral agent and making it accessible to virtually all pancreatic cancer patients with KRAS mutations rather than a narrow subtype. This is why RASolute 302 showed consistent HR 0.40 benefit regardless of KRAS variant subtype, and why the results are properly described as broad-spectrum RAS(ON) inhibition rather than targeted inhibition of a single mutation — the science of the mechanism matches the breadth of the clinical benefit. The significance extends beyond pancreatic cancer: demonstrating that broad RAS inhibition is pharmacologically achievable opens a conceptual and practical path toward treating the much larger populations of KRAS-mutant lung and colorectal cancer patients with similar broad-spectrum approaches. In my view, establishing the proof of concept for broad-spectrum RAS inhibition is the most important scientific contribution daraxonrasib makes — one that will generate decades of downstream clinical development regardless of what happens to this individual molecule.
- Unlocking 60+ Pipeline Drugs and an Entire Research Era
Daraxonrasib's Phase 3 success has catalytic effects that extend well beyond a single drug's approval — it validates a therapeutic hypothesis that had been blocked for decades by the "undruggable" label, and that validation has already accelerated investment in more than 60 RAS-targeted compounds currently in clinical development worldwide, spanning not just RAS(ON) inhibitors but SHP2 inhibitors, SOS1 inhibitors, RAF dimer inhibitors, and combination immunotherapy strategies. Among the most advanced competitors, MRTX1133 (Mirati/Bristol-Myers Squibb) is a G12D-specific inhibitor already in Phase 1/2 testing, and the forthcoming comparison of broad-spectrum versus mutation-specific RAS inhibition will generate important scientific data about which patient populations benefit most from each approach — competition that ultimately serves patients by expanding available options. Revolution Medicines' own RASolute 303 first-line Phase 3, which began enrolling approximately 900 patients in April 2026, represents the immediate next expansion of the daraxonrasib platform, and the Phase 1/2 combination therapy data (ORR 58%, disease control rate 90%, six-month OS 90%) provides a credible empirical foundation for expecting a meaningful first-line result. For researchers and clinicians who spent 40 years being told this target was impossible, the current pipeline represents an extraordinary intellectual and commercial correction of a long-standing scientific blind spot — one that was maintained not because the problem was fundamentally unsolvable, but because it was fundamentally underfunded. The breadth and speed of the current development ecosystem suggests that the field is now moving with urgency proportionate to the clinical need.
- FDA 48-Hour Expanded Access Approval — Urgency Recognized at the Regulatory Level
The FDA's decision to approve expanded access for daraxonrasib within 48 hours of receiving the application on April 28, 2026 — granting approval on April 30 — is an unusual response even by Breakthrough Therapy standards, reflecting how clearly the agency read the Phase 3 data's clinical significance for a disease with catastrophically limited second-line treatment options. In addition to the expanded access decision, the FDA has granted daraxonrasib a triple combination of regulatory advantages: Breakthrough Therapy designation that expedites development collaboration with FDA, Orphan Drug designation that provides market exclusivity incentives, and the Commissioner's National Priority Voucher that substantially reduces NDA review timelines for conditions of major public health urgency. These three designations awarded simultaneously to a single drug are genuinely rare, signaling that the FDA views daraxonrasib not as a marginal improvement but as a categorically new option in a severely underserved disease area where the agency is willing to use every available tool to accelerate access. The Commissioner's National Priority Voucher in particular is a mechanism designed specifically to fast-track NDA review for diseases of exceptional unmet need, and its award here makes a first-half 2027 formal approval timeline substantially more achievable than standard procedures would allow. For the estimated 18,000 Americans diagnosed annually with second-line metastatic pancreatic adenocarcinoma, the practical implication is that the pathway from current expanded-access availability to full insurance-covered standard prescription is compressed more tightly than for almost any other drug currently in the approval pipeline.
Concerns
- A Price Wall That Makes This a Breakthrough Only for the Wealthy
The Stifel-estimated monthly price of $30,547–$37,318, representing an annual cost of $237,556–$269,051 per patient, is nearly double the monthly cost of sotorasib and positions daraxonrasib as one of the most expensive oncology drugs in any category — with the premium justified by Revolution Medicines on the basis of broader mutation coverage and dramatically superior survival data relative to standard second-line chemotherapy. In the United States, this price level almost certainly triggers Medicare Inflation Reduction Act price negotiation pressure, and large private insurers will deploy prior authorization and step-therapy requirements that create significant administrative friction even for patients who nominally have coverage for the drug. The global dimension is far starker: a systematic review published in Frontiers in Public Health found that 57.7% of anti-cancer medicines in low-income countries are entirely out-of-pocket expenses, with 8.3% not available at all; in Bangladesh, where 84% of households earn $2–9 per day, average cancer treatment costs total $3,234 per treatment course — a $37,000 monthly drug simply does not exist in that economic reality as a treatment option. Nature Reviews Clinical Oncology has documented that more than 50% of WHO essential medicines list anti-cancer drugs are already inaccessible in low- and middle-income countries; daraxonrasib, at its projected price, will exceed that accessibility threshold by an order of magnitude. I believe this pricing structure creates a genuine ethical obligation to negotiate tiered pricing agreements or generic licensing arrangements that extend meaningful access beyond wealthy nations — an obligation made more pressing, not less, by the extent to which decades of publicly funded research enabled this drug's development.
- Multiple Resistance Mechanisms Already Documented — Long-Term Durability Uncertain
Research presented at AACR has identified several distinct acquired resistance mechanisms in patients receiving daraxonrasib monotherapy: KRAS gene amplification observed in three patients, MAP2K1/2 mutations in five patients, and PI3K/MTOR pathway alterations in four patients, alongside preclinical evidence of KRAS Y64X and Y71H secondary mutations, Myc amplification, and RAF dimerization changes that may represent additional clinical resistance routes. These resistance mechanisms primarily operate through reactivation of the RAS–MAPK signaling pathway, and in cases involving receptor tyrosine kinase upregulation, they may require combination strategies targeting EGFR or MET to suppress the most active escape pathways. A 2026 Cell paper raised the additional concern that molecular glue complex disruption may represent a resistance mechanism applicable to the entire class of RAS(ON) inhibitors — not just daraxonrasib — which means the resistance problem may be structural to the therapeutic approach rather than addressable through minor modifications to a single drug. The current 13.2-month median overall survival reflects single-agent performance in a trial population that has not accumulated enough follow-up time to fully reveal what the durable response profile looks like, and whether the survival benefit concentrates in a biomarker-identifiable responder subpopulation will only be known through longer follow-up data unavailable before 2028 or later. I think this means the "game changer" label should be held as conditional — fully valid as a proof of concept and as a first step, but genuinely contingent on combination strategies successfully managing the resistance pathways that have already been identified in early post-approval experience.
- 13.2 Months Is Still a Death Sentence — The Danger of Overhyped Rhetoric
The terms "game changer," "grand slam," and "revolution" — employed by clinicians at ASCO and amplified across media coverage — risk creating a version of hope that the current evidence cannot sustain for a disease where the five-year survival rate remains approximately 10% and where the Phase 3 data does not yet include mature long-term follow-up showing whether any patient subpopulation achieves genuinely durable survival. Dr. Anirban Maitra at NYU Langone Health has been emphatic and public about the risk of misinterpretation: "This is not a cure. We have not cured pancreatic cancer. I cannot emphasize this enough." Dr. Elizabeth Jaffee at Johns Hopkins similarly noted that despite decades of developing new therapies for this disease, it "is still a death sentence" — statements that should be given equal prominence alongside the enthusiastic clinical response at ASCO. When "survival doubled" becomes conflated in popular understanding with "pancreatic cancer solved," patients and families face the psychological harm of hope built on a fundamental misunderstanding — and that harm is intensified rather than mitigated by the legitimate scientific excitement that genuinely impressive data deserves. Revolution Medicines' stock price at approximately 10x its IPO lows, and the $2.225 billion secondary offering that followed the ASCO presentation, reflect investor confidence in the commercial opportunity; for the patients these numbers ultimately concern, however, calibrated honesty about what 13.2 months means in the context of a still-fatal disease is more valuable than any amount of market enthusiasm.
- First-Line Expansion Is Unproven — RASolute 303 Results Still Years Away
The single most important open question for daraxonrasib's long-term clinical profile is whether the dramatic second-line effect size (HR 0.40) translates to the first-line setting — and the answer won't arrive before 2028 or 2029 at the earliest, leaving a substantial period of uncertainty between the current Phase 3 success and the drug's ultimate profile. RASolute 303 enrolled its first patient in April 2026 and will require approximately 900 patients across monotherapy and combination arms, a sample size and event accumulation requirement that places the primary endpoint readout minimum two to three years from now under optimistic enrollment assumptions. The Phase 1/2 combination data (ORR 58%, DCR 90%) is directionally encouraging but was generated in small, early-phase cohorts with all the limitations that entails — selection effects, short follow-up, and no randomized comparator — and cannot reliably predict Phase 3 outcomes in an unselected first-line patient population. The first-line setting also involves a substantially longer expected treatment duration than the second-line context in which the Phase 3 data was generated, meaning that the adverse event profile — rash in 86% of patients and stomatitis in 54% — will need to be managed over longer treatment courses, and cumulative toxicity effects that are acceptable over a 7-month median PFS may become more clinically significant over a 12-month-plus first-line course. I believe first-line approval is the most likely next chapter for daraxonrasib — but that confidence is grounded in the strength of the second-line data and early-phase signals, not in proven Phase 3 first-line outcomes, and investors and patients should hold both the optimism and the uncertainty simultaneously rather than assuming the transition is automatic.
- Public Research Funding Generates Private Pricing Power — A Structural Design Problem
The scientific foundation that made daraxonrasib possible rests substantially on decades of publicly funded research: NCI investment in basic KRAS biology going back to the 1980s, the NCI RAS Initiative established in 2013, university laboratory programs funded by government grants across multiple countries, and public regulatory instruments — Breakthrough Therapy designation, Orphan Drug status, and the Commissioner's National Priority Voucher — that actively de-risked and accelerated the development timeline. Revolution Medicines' private investment in late-stage clinical development, trial operations, regulatory submission, and manufacturing scale-up is real and substantial, and the company's shareholders accepted genuine financial risk during the years before Phase 3 data confirmed efficacy; these contributions deserve acknowledgment and appropriate reward. But the conversion of substantially publicly funded foundational science into a $37,000-per-month product accessible to a small fraction of the world's pancreatic cancer patients raises a structural question that extends beyond any individual company's pricing decisions: at what point does public investment in the research commons create an obligation regarding access that private commercial rights do not supersede? The $8,945 in per-death NCI research investment that American taxpayers made toward pancreatic cancer science — while breast cancer received $69,800 per death — has produced a drug that sits behind a monthly price barrier exceeding most Americans' monthly household income. I don't think Revolution Medicines is uniquely culpable in a system that systematically converts public basic research into private pricing power across the industry; I think the system's design itself is the failure that daraxonrasib's success makes more visible, not less, and that visibility creates both the opportunity and the obligation to address it.
Outlook
The most pressing near-term milestone is Revolution Medicines' submission of a New Drug Application to the FDA for daraxonrasib. The drug already holds Breakthrough Therapy designation, Orphan Drug designation, and a Commissioner's National Priority Voucher — a combination of regulatory advantages that can substantially compress the standard review timeline. I expect the NDA to be filed in the second half of 2026, with Priority Review designation following, and a realistic pathway to formal FDA approval in the first half of 2027. The FDA's 48-hour turnaround on the expanded access application in late April 2026 — from filing on the 28th to approval on the 30th — signals that the agency is moving with the clinical urgency this disease demands. Formal approval is what converts the current expanded-access pathway into standard insurance coverage for the estimated 18,000 Americans diagnosed annually with second-line metastatic pancreatic adenocarcinoma, and the Commissioner's National Priority Voucher makes that 2027 timeline substantially more achievable than standard procedures would allow.
The drug pricing negotiation dynamics represent the most significant near-term headwind to commercial momentum. The Stifel-estimated monthly price of $30,547–$37,318 is nearly double the monthly cost of sotorasib, and at that level, daraxonrasib will almost certainly attract Medicare price negotiation pressure under the Inflation Reduction Act's strengthened drug pricing provisions. Revolution Medicines will argue that the breadth of mutation coverage and the magnitude of survival benefit justify the premium, and from a health economics standpoint, a drug producing HR 0.40 in second-line pancreatic cancer has a defensible value proposition in the American market. But the political environment around pharmaceutical pricing has shifted considerably, and large private insurers are increasingly deploying prior authorization requirements and step-therapy mandates as de facto price controls. I expect the effective realized price per patient in the U.S. to settle meaningfully below the list price over time — though the trajectory of that convergence will depend heavily on how aggressively CMS exercises its new negotiation authority.
The RASolute 303 Phase 3 trial is the second major near-term signal to monitor closely. The first patient was dosed in April 2026, with approximately 900 patients planned across daraxonrasib monotherapy and daraxonrasib combined with gemcitabine and nab-paclitaxel — the current first-line standard of care. I believe enrollment will proceed faster than typical for a pancreatic cancer indication. The second-line Phase 3 data was so compelling that patients and oncologists seeking trial access will drive aggressive participation at sites already running established RASolute 302 operational infrastructure. Full results from RASolute 303 will not arrive before 2028 at the earliest, but interim analyses and safety data presented at conferences along the way will shape clinical practice patterns and market expectations well before the primary endpoint readout. How quickly the trial completes enrollment will itself become a meaningful leading indicator.
Phase 1/2 combination therapy preliminary data has already produced numbers that make the first-line case look credible: an objective response rate of 58%, a disease control rate of 90%, a six-month progression-free survival rate of 84%, and a six-month overall survival rate of 90%. These are striking signals for a first-line pancreatic setting where the current standard of care (gemcitabine plus nab-paclitaxel) produces a median overall survival of approximately 8.5 months and a one-year survival rate under 35%. I want to be appropriately cautious here — this is early-phase, small-cohort data, and small Phase 1/2 cohorts in pancreatic cancer have disappointed in large randomized Phase 3 settings many times before. But the direction is consistent with what a drug of daraxonrasib's demonstrated second-line potency should theoretically be capable of in the first-line setting, and it provides scientific rationale for sustained optimism about RASolute 303.
Looking at the medium-term landscape from 2027 through 2028, the competitive dynamics around daraxonrasib will take meaningful shape. MRTX1133, the KRAS G12D-specific inhibitor now part of Bristol-Myers Squibb following the Mirati acquisition, is progressing through Phase 1/2 and could reach Phase 3 readiness by 2027. The clinical distinction matters: daraxonrasib's broad-spectrum approach covers G12D, G12V, and G12R simultaneously, while MRTX1133 targets G12D specifically — the single most common KRAS variant in pancreatic cancer at 40%. For G12D-dominant tumors, a selective inhibitor might achieve a cleaner pharmacological profile; for tumors with mixed KRAS variants, the broad-spectrum approach likely wins. I expect this differentiation to generate productive scientific competition rather than zero-sum displacement. More than 60 RAS-targeted drugs are in development globally, including SHP2 inhibitors, SOS1 inhibitors, and RAF inhibitors being explored specifically as combination partners to address known resistance mechanisms — and the 2027–2028 window will see the first meaningful Phase 2 readouts from many of these programs.
Resistance is, in my view, the single most important variable determining daraxonrasib's long-term impact — and the one most likely to complicate the current "game changer" framing. Research presented at AACR has already documented acquired resistance mechanisms in patients on daraxonrasib monotherapy: KRAS amplification in three patients, MAP2K1/2 mutations in five, and PI3K/MTOR pathway alterations in four. A 2026 paper published in Cell identified molecular glue complex disruption as a resistance mechanism that may not be specific to daraxonrasib but could apply to the entire class of RAS(ON) inhibitors — a broader structural concern for the field. By 2028, patients who began daraxonrasib in 2026 or 2027 will have longitudinal follow-up data revealing how the survival curve evolves beyond the current 13.2-month median. If the curve's tail is encouragingly long, it validates the current optimism. If resistance emerges broadly and drives the survival curve toward the chemotherapy arm at 18–24 months, the urgency of combination strategies increases substantially and the monotherapy's commercial ceiling compresses. The precedent of sotorasib — whose real-world durable benefit proved narrower than initial Phase 2 enthusiasm suggested — makes this a scenario to take seriously rather than dismiss.
Looking out to 2028 through 2031, the potentially transformational development for daraxonrasib is indication expansion beyond pancreatic cancer. KRAS mutations appear in roughly 25% of non-small cell lung cancers and 40–50% of colorectal cancers — two of the most common cancers globally — making these the most important potential expansion opportunities. Market analyst projections for daraxonrasib's peak annual revenue in pancreatic cancer alone run to $5–8.5 billion. Successful expansion into lung and colorectal settings could push peak revenue above $10 billion, placing daraxonrasib among the top-tier global pharmaceutical blockbusters. I believe indication expansion is the most likely long-term development pathway — but each new cancer type requires its own dedicated Phase 3 trial, and the tumor microenvironment, co-mutation landscape, and established treatment sequences in lung and colorectal cancer differ meaningfully from pancreatic cancer. The expansion is not automatic, and assuming smooth translation from the pancreatic Phase 3 success would be a significant analytical error.
The demographic backdrop for all of these projections is one of accelerating need. A 2026 Journal of Global Health analysis projects global pancreatic cancer incidence to increase 95.4% by 2050, reaching approximately 998,663 cases annually — driven by aging populations, rising obesity rates, and increasing type 2 diabetes prevalence worldwide. In the United States, pancreatic cancer is forecast to overtake colorectal cancer as the second leading cause of cancer death by 2030. This epidemiological tide is rising precisely as effective targeted therapies are becoming available for the first time. The structural irony is that incidence is growing fastest in low- and middle-income regions where a $37,000-per-month drug is not a pricing discussion but a categorical impossibility. Without deliberate policy intervention, the gap between what science can do and what reaches most patients will widen even as the science improves.
I believe structural policy solutions are becoming increasingly inevitable, though their timeline remains uncertain. The combination of rising incidence, dramatic survival benefit, and extreme pricing creates political and policy pressure that will be difficult to contain through the 2030s. Compulsory licensing — permitting generic manufacturers to produce a drug without the patent holder's consent in exchange for royalties — is explicitly authorized under the World Trade Organization's TRIPS Agreement for public health emergencies, and arguments for its application to daraxonrasib in high-burden, low-resource settings will eventually be made in multilateral forums. Tiered pricing agreements, where pharmaceutical companies offer substantially reduced prices in low- and middle-income countries in exchange for re-importation restrictions, represent a less confrontational middle path that some companies have adopted for HIV medications without compromising global profitability. I expect both mechanisms to become live regulatory and political debates before 2030, and their resolution will determine whether daraxonrasib's scientific achievement ultimately translates into meaningful global health impact or remains accessible only to a small fraction of the world's patients.
In the bull-case scenario, FDA approval arrives in the first half of 2027 with manageable pricing friction; RASolute 303 first-line results in 2028–2029 demonstrate a hazard ratio in the 0.45–0.50 range, confirming the second-line effect translates to the first-line setting; lung and colorectal indication programs reach Phase 3 enrollment by 2029–2030 and deliver preliminary results by 2031; and peak annual revenue exceeds $8.5 billion. The Commissioner's National Priority Voucher and Breakthrough Therapy designation make the FDA timeline plausible, the Phase 1/2 combination data (ORR 58%, six-month OS 90%) provides empirical foundation for first-line optimism, and a tiered pricing agreement by 2029 partially addresses the global equity gap. This scenario is supported by the extraordinary strength of the Phase 3 data — an HR of 0.40 with p=4.6×10⁻¹¹ rarely fails to generate downstream regulatory momentum.
In the base case, FDA approval comes in 2027; first-line RASolute 303 results arrive in 2029 with a solid but smaller effect size than second-line (HR around 0.52–0.58); indication expansions into lung and colorectal cancer proceed methodically but face meaningful competition from mutation-specific inhibitors; acquired resistance data shows that durable benefit concentrates in a biomarker-identifiable responder subpopulation; and peak annual revenue stabilizes in the $5–7 billion range. In the bear case, acquired resistance mechanisms emerge more broadly and rapidly than current data suggests, affecting the majority of second-line patients within 12–15 months, and the durable survival tail proves limited to a small subset. First-line RASolute 303 data disappoints with HR 0.65 or higher. Aggressive Medicare price negotiation compresses realized prices enough to dampen U.S. commercial uptake, and peak revenue falls below $3 billion. This is not the most likely outcome, but the sotorasib precedent makes it a scenario to hold with intellectual honesty rather than dismiss on the basis of Phase 3 enthusiasm alone.
Finally, let me be transparent about what could invalidate my forecast. My strongest concern is resistance, and that concern could resolve more favorably than I expect if combination therapy strategies — daraxonrasib plus SHP2 inhibitor, plus EGFR inhibitor, or plus immunotherapy — produce durable Phase 2 responses in 2027 that demonstrate effective management of the identified resistance pathways. Conversely, if political pressure on pharmaceutical pricing proves faster and stronger than I project — if the U.S. government or major European authorities negotiate or mandate prices toward $10,000–$15,000 per month — global access could improve more rapidly than my current estimates suggest. Whatever scenario plays out, one thing is fixed: daraxonrasib has made the "undruggable" druggable, and the scientific momentum that follows from that proof of concept will reshape oncology regardless of what happens to this particular molecule. If you or a loved one is living with pancreatic cancer, please work closely with your oncologist to explore eligibility for the expanded access program or the RASolute 303 trial. Treatment effects vary by individual, and all decisions must be guided by a physician who knows your full clinical picture.
Sources / References
- Daraxonrasib or Chemotherapy in Previously Treated Metastatic Pancreatic Cancer — New England Journal of Medicine (Phase 3 RASolute 302 Full Results)
- Multi-Selective RAS Inhibitor Nearly Doubles Survival in Pancreatic Cancer — American Society of Clinical Oncology, ASCO 2026
- RAS(ON) Inhibitor Doubles Median Overall Survival in Phase 3 Trial for Patients with Metastatic Pancreatic Cancer — Dana-Farber Cancer Institute
- Incidence, Mortality, and Federal Research Funding by Cancer Type — PubMed Central / NCI Cancer Research Funding Analysis (2025)
- FDA Permits Expanded Access for Investigational Pancreatic Cancer Drug — U.S. Food and Drug Administration
- Availability, Affordability, and Pricing of Anti-cancer Medicines in Low- and Middle-Income Countries — Frontiers in Public Health / PubMed Central
- Disrupted Molecular Glue Complex Drives RAS Inhibitor Resistance — Cell (2026)
- First RAS Inhibitor Extends Survival in Previously Treated Metastatic Pancreatic Adenocarcinoma — Pancreatic Cancer Action Network (PanCAN)
- Drugging the 'Undruggable' KRAS: From Discovery to Clinical Landscape — PubMed Central / Cancer Biology & Medicine
- Global Surge in Pancreatic Cancer Cases: Epidemiological Projections Through 2050 — Journal of Global Health (2026)